Breaking Down Barriers: How Administrative Friction Puts Medicaid Access at Risk
Every hour a provider spends navigating paperwork is an hour taken away from patient care. As care delivery models grow more complex, healthcare providers face mounting administrative hurdles. This goes beyond mere inconvenience, creating a structural barrier to care access within state Medicaid programs.
Recent data reveals the depth of this challenge. In partnership with a third-party research firm, Gainwell surveyed hundreds of medical providers to understand their experience with Medicaid operations. The findings show that complex billing, credentialing, and enrollment processes directly undermine network stability.
Provider Satisfaction as an Indicator of Network Stability
Every extra form, stalled approval, or rejected claim sets off a negative chain reaction for medical practices. It means another delay in treating patients, reduced access to care, and disruption in reimbursement. These ongoing challenges erode provider satisfaction, with nearly one-third of providers reporting they are dissatisfied with current Medicaid administrative processes.
The impact is most severe where access is already fragile. Behavioral health providers report being 75% more dissatisfied with administrative tasks than their peers, reflecting the disproportionate burden placed on specialty and high-need care settings.
For small and independent practices, the strain is even greater. With limited administrative staff, these providers absorb complexity directly. Time that should be spent caring for patients—especially individuals with mental health needs—is instead consumed by tracking credentialing changes, appealing denials, and navigating opaque state systems. Administrative work crowds out clinical care. Frustration with administrative tasks quickly translates into business decisions that limit care. Dissatisfied providers often alter their participation in Medicaid.
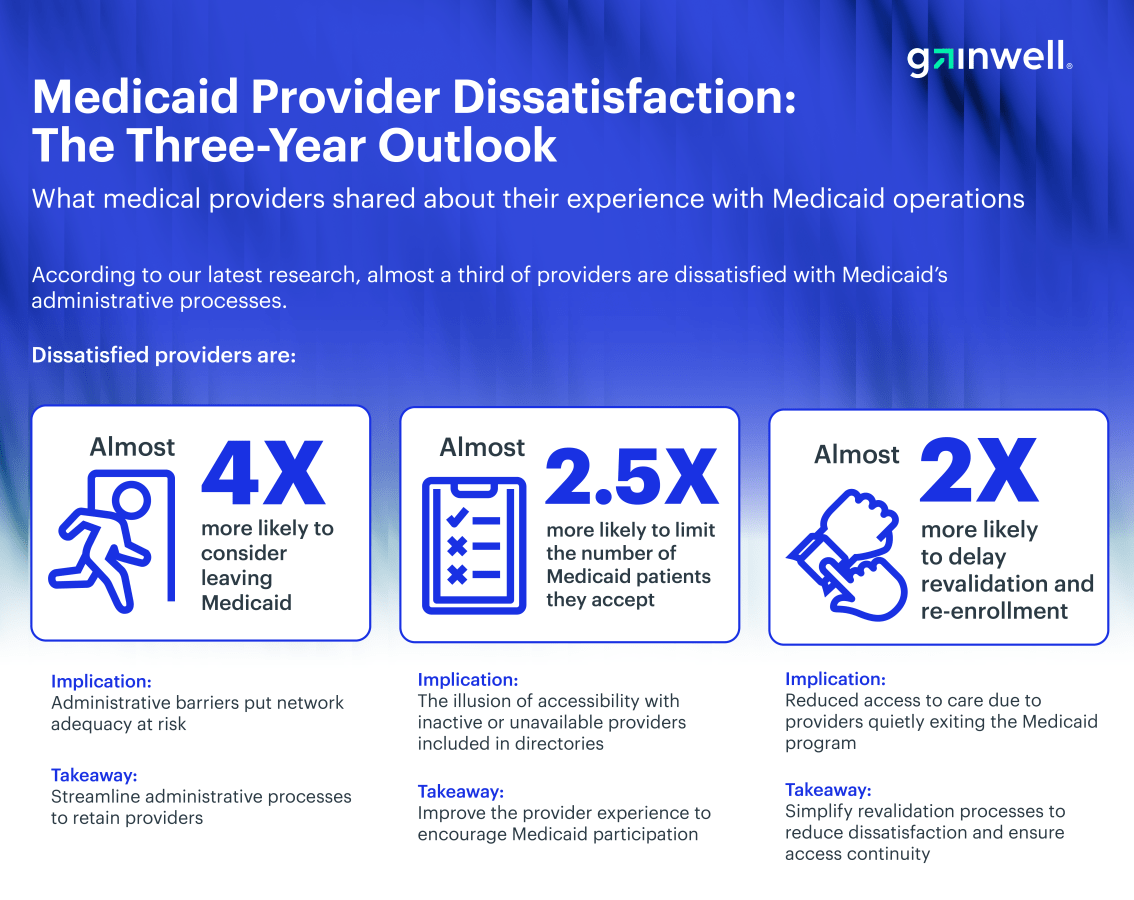
Compared to their satisfied peers, dissatisfied providers are almost four times more likely to consider leaving Medicaid. Even when they remain in the network, the friction takes a toll. Frustrated providers are nearly 2.5 times more likely to limit the number of Medicaid patients they accept. They are also twice as likely to delay revalidation and re-enrollment, which can result in administrative termination.
With the recent CMS announcement mandating more frequent and rigorous revalidation processes, states must consider how this could further impact network adequacy and consider ways to curb provider churn in their two-year provider revalidation strategies.
Provider churn contributes to the rise of ghost provider networks, where directories list inactive or unavailable providers, creating an illusion of accessibility. For patients, especially those in rural areas or requiring specialty care, these inaccuracies have serious consequences. Searching for a provider turns into a frustrating and time-consuming process, with many patients facing repeated dead ends. This not only delays access to necessary care but also heightens the challenges for populations already grappling with social and geographic barriers to health services.
The impact is particularly stark for Medicaid beneficiaries, who may have fewer alternatives and are more reliant on accurate directories to meet their urgent healthcare needs. Without intervention, ghost networks perpetuate inequities, leaving vulnerable individuals underserved and eroding trust in the system.
Shrinking Networks and Patient Access Risks
These choices can accumulate, quietly eroding the stability of the Medicaid network. Network adequacy depends on providers who are not just enrolled, but actively willing to participate. When administrative roadblocks push providers to cap their panels or exit the program, the safety net shrinks.
The data makes it clear that reducing administrative burden is a core access strategy. State agencies are accountable for network adequacy and quality of care; if a state fails to alleviate these burdens, it can unintentionally reduce patient access to essential services even as demand continues to rise. An inefficient system often signals to the medical community that their time is not valued, making it harder for Medicaid to compete with commercial plans for provider participation.
Building a Modern and Stable Medicaid Network
The data offers a clear path forward. Providers in states with modernized, integrated enrollment and credentialing systems report 50% higher satisfaction than those without.
Providers want consolidated workflows. Specifically, 72% of providers would prefer a single credentialing application across all managed care organizations (MCOs) and states. They also showed value in 24-hour claim status visibility and faster enrollment approvals.
Transforming the Medicaid provider experience is not just an opportunity—it is an imperative for states aiming to retain a strong provider network and ensure continuity of care. Ultimately, states must view backend systems as provider engagement platforms. To achieve this, states must prioritize modernization efforts with a clear and structured approach that addresses pain points in their existing systems. Indecisiveness or lack of action risks further exacerbating provider dissatisfaction and weakening the safety net that many rely on.
The starting point for these efforts should be a comprehensive gap analysis of credentialing and enrollment workflows. States must assess their current processes to uncover inefficiencies and bottlenecks. To gain deeper insights, engaging providers directly through surveys or focus groups is essential to identify exactly where they experience the most friction. This feedback is a critical resource to guide the transformation process.
States must take analysis and provider findings and use them to build a modernization strategy that streamlines workflows, reduces administrative burdens, and fosters a more provider-friendly system. By taking these steps, states can safeguard Medicaid more effectively, reinforce provider participation, and uphold the promise of care for their most vulnerable populations.





